

.jpg)
Familial hypercholesterolaemia (FH) affects approximately 1 in 250 Australians, yet up to 90% of individuals remain undiagnosed, representing a significant missed opportunity for early cardiovascular risk reduction.
FH is an autosomal dominant inherited disorder characterised by markedly elevated low-density lipoprotein cholesterol (LDL-C) from an early age. It is frequently under-recognised and may be misclassified as polygenic or lifestyle-related hypercholesterolaemia, despite requiring distinct and more intensive management.
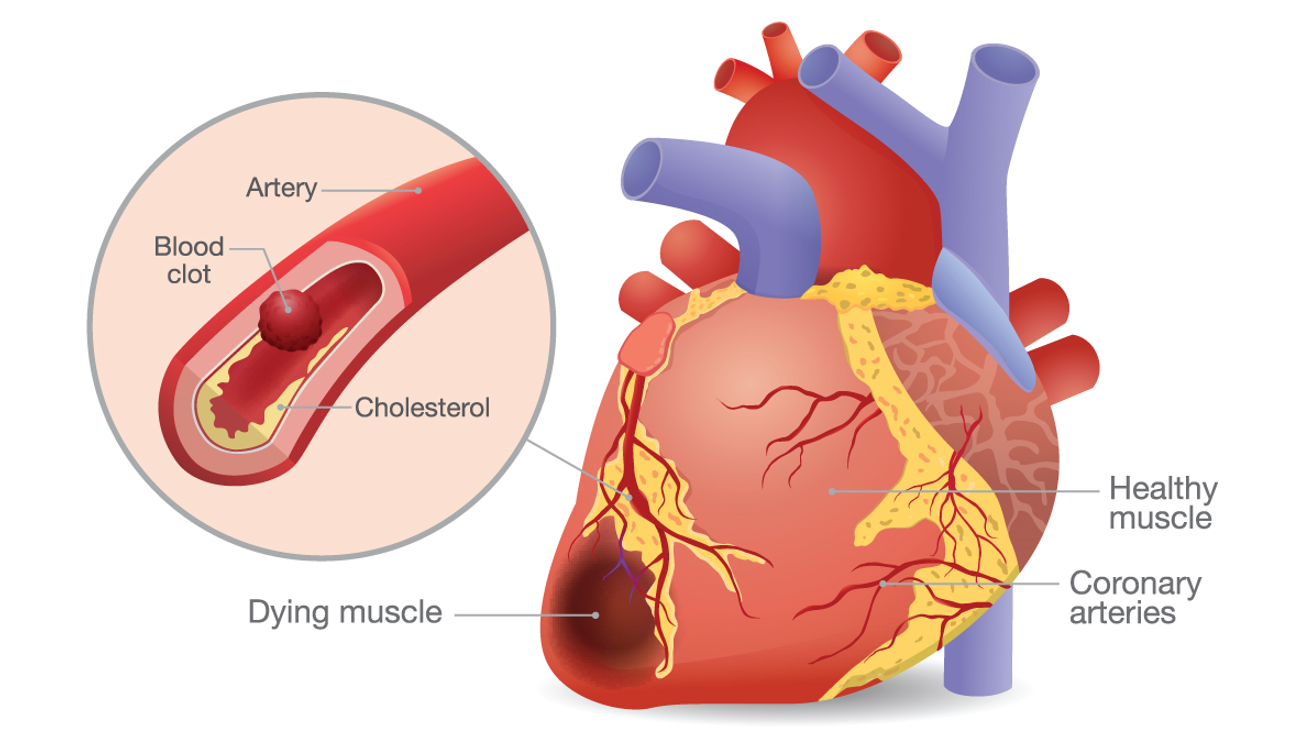
Untreated FH is associated with a significantly increased risk of premature atherosclerotic cardiovascular disease:
Early identification and treatment can substantially reduce morbidity and mortality.
This assay analyses a 9-gene panel associated with FH and related lipid disorders.
The majority of pathogenic variants are identified in:
Genetic testing for FH may be performed in two key scenarios:
Where a familial variant is identified, Genomic Diagnostics offers targeted single-gene testing for at-risk relatives, supporting streamlined cascade testing. This testing may be eligible for Medicare rebate where clinical criteria are met, and can be requested by a GP or specialist with appropriate clinical information, supporting cost-effective family screening.
Genetic testing supports the diagnosis and management of FHand has several important clinical applications:
Testing should be considered in patients with:
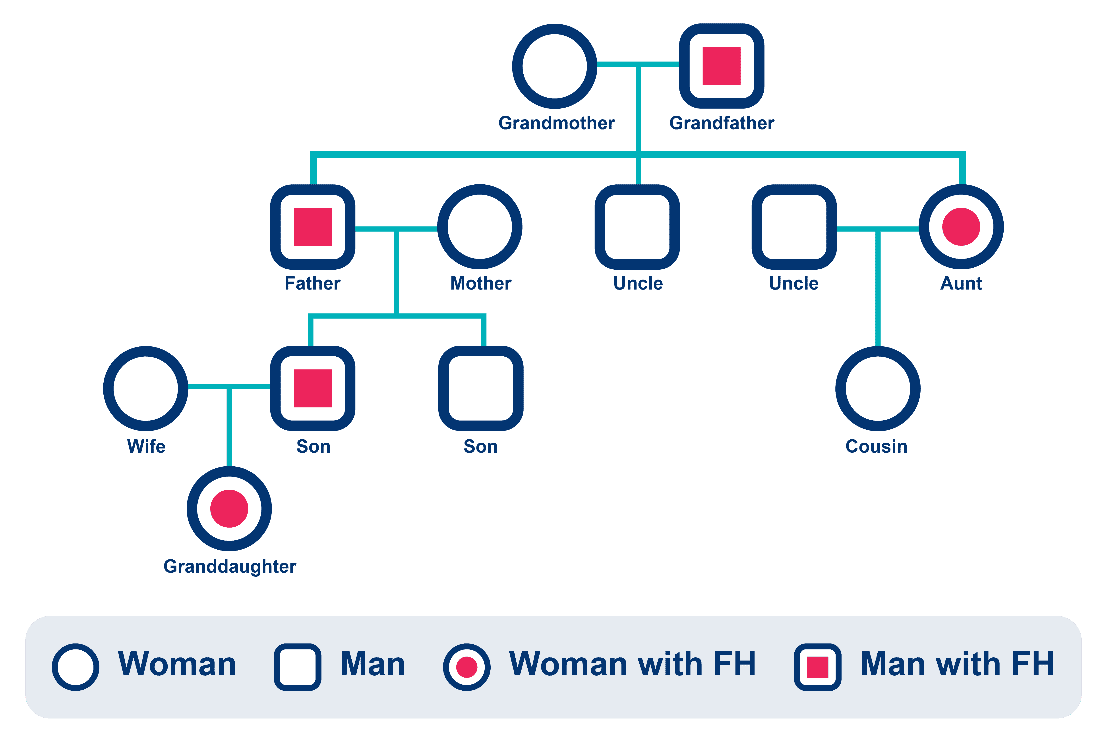
FH is inherited in an autosomal dominant manner. First-degree relatives have a 50% probability of carrying the variant, supporting targeted cascade testing.









Birkenhead K et al. Familial hypercholesterolaemia in Australia. Medicine Today, 2023.
Reamy BV. Familial Hypercholesterolemia: Screening, Diagnosis, and Treatment. AAFP, 2024.